Overall aims and objectives of the projects
Main target of the present proposal is the realization of the OPTIMO sensor, a portable device based on an all-optical technology capable to perform manometry, pH-metry and bilimetry within the same optical fiber catheter or by means of combined catheters to provide physicians with a compact and reliable tool to perform exhaustive diagnosis in gastroesophageal reflux pathologies.
Present technology allows the measurement of these three important esophageal parameters – i.e. pressure, pH and bile – based on different technologies and by means of separate catheters each of them with a diameter of the order of mm (e.g. 1 mm for pH, 3.7 mm for bile and 2.5 or more for manometry) and connected to different portable devices. This often prevents the possibility of their simultaneous measurement on the same patient over the 24-hour measurements and, in any case, it creates, if performed, a not negligible discomfort to patients.
The OPTIMO sensor based on an all-optical technology and offering the possibility of performing the measurement of the three parameters simultaneously by means of the use of a single or combined catheter would be definitely an innovative product in the gastroesophageal diagnostic scenario with high potential for worldwide market penetration and application developments.
The achievement of this main target implies the accomplishment of the following objectives:
- development of the optical fiber sensor for the measurement of pH;
- development of the optical fiber sensor for bile detection;
- development of the optical fiber manometer;
- integration of the optical fiber sensors within a single catheter;
- realization of the portable interrogation unit for all the three parameters;
- clinical assessment of the whole device on volunteers and on patients.
In the design and development of the three different optical fiber sensors, one of the main requirements is given by the necessity of coupling all of them within a single catheter, considering also the need of a relatively simple fabrication process.
In order to replace a device in use in clinical practice for many years, it is clear that the proposed optical sensors must be characterized by equal or superior performances. This leads to very specific requirements that are summarized in Table below.
Parameter | Project target | State of the art | |
Manometer | Pressure range | 0-375 mmHg | 0-200 mmHg |
Pressure resolution | 1 mmHg | 1 mmHg | |
Spatial range | 30 cm | 20 cm – 30 cm | |
Spatial resolution | 2.5 cm | 10 cm – 1 cm | |
pH sensor | Measurement Range | 1-8 pH units | 1-8 pH units |
Accuracy | 0.05 pH units | 0.1 pH units | |
Response time | ≤ 20 s | 10-30 s | |
Bile sensor
| Measurement Range | 0-1 absorbance unit | 0-1 absorbance unit |
Accuracy | 5% | 5% | |
Response time | 10 s | 10 s | |
Overall parameters | Diameter | < 4.8 mm | no combined catheter exist |
Measurement time | 24 h | 24 h |
Scientific, technical and commercial challenges
Different challenges can be identified in the proposed project.
From a scientific point of view, the identification of a correct scientific approach for the integration of the three different sensors in a single catheter is absolutely not trivial, being the detection principle used for the measurement of bile and pH, on one side, and pressure monitoring, on the other, completely different:
- modulation of the optical intensity carried by the optical fiber for bile and pH due to the change of optical absorption induced by bilirubin the main biliary pigment and by an acid-base indicator for bile and pH detection, respectively;
- wavelength shift of the reflected peaks transmitted by fiber Bragg gratings (FBGs) induced by esophageal pressure changes.
In terms of technical challenges, surely, the highest one is strictly correlated to the previous one, since, whichever is the scientific approach identified, it must lead to the implementation of a reasonable fabrication process characterized by an acceptable fabrication cost.
Actually, the different optical fiber sensors, developed separately by some of the partner of the project must be largely or completely redesigned in order to allow the accomplishment of the final objective of a completely integrated catheter for the simultaneous measurement of the three parameters.
Another not negligible technical challenge is associated with the fact that the developed OPTIMO device must be a portable POC device capable to perform a 24-hour monitoring of the three parameters.
As a matter of fact, the mandatory requirement coming from the physicians is that this 24-hour monitoring must not imply the hospitalization of the patient, who, on the contrary, should be able to go home after the insertion/positioning of the catheter and then to come back the day after for the catheter removal, being this the standard procedure followed for the separate monitoring of the three parameters.
This implies that the optoelectronic sub-modules for the interrogation are compact and portable. If this is relatively easy for the absorption based sensors (bile and pH) thanks to the use of very powerful light emitting diodes and very efficient photodetectors, the same cannot be said for pressure monitoring for which extremely sensitive spectrum analyzers capable to detect wavelength shift at sub-nanometer and wavelength division multiplexing techniques are necessary for the pressure detection on different locations along the same optical fiber.
Commercial challenges are mainly associated to the capability of market penetration by the consortium in the area of POCT device.
As a general claim, it should be noted that, even in the case of a completely successful project, there would be still a distance to the market that is mainly associated to the completion of the clinical assessment of the OPTIMO device and to its clinical validation, which will have to be performed on a sufficiently high number of patients.
State of the art - Current level of the knowledge
Gastroesophageal reflux disease (GERD) is very common pathology, which affects between 10% and 20% of the western population.
The esophagus is a hollow tube, which transports food from the mouth to the stomach. Anatomically, it is a simple tube with sphincters at both ends.
The sphincters function to keep the tube empty from external (food) and internal (acid) intrusions.
Swallowing and transport of food from the mouth to the stomach is a highly coordinated neuromuscular event.
Dysfunction of the peristaltic transport mechanism causes a variety of diseases like GERD, esophageal adenocarcinoma, heartburn or pyrosis, achalasia and nutcracker esophagus.
When the clinical picture remains unclear, the functionality of the esophagus has to be examined with sensors.
A clearly defined goal is to make these examinations faster and more comfortable to the patient.
In order to have a correct clinical picture and in order to be able to perform a correct diagnosis, the measurement of more than one parameter in the gastroesophageal apparatus is necessary, mainly esophageal pressure, pH and bile, which are measured at ambulatory level with portable instrumentation.
The measurement of pH in the stomach and the esophagus (gastroesophageal pH monitoring) is a universally accepted practice and extremely widespread in the clinical field for the diagnosis of gastroesophageal reflux disorders in the apparatus since the 80’s. pH is generally measured in two positions: in correspondence of the lower esophageal sphincter (LES) and five cm above it.
The measurement is normally made via a mini-pH electrode positioned in the esophagus and/or stomach.
This type of analysis, known as pH-metry, generally has a duration of 24 hours and is an outpatient measure, with the probe positioned in the esophagus and/or stomach of the patient who is then sent back at home.
The day after the patient comes back to the hospital for the removal of the probe. This implies that the measuring device is portable and powered by batteries that can record the data for the entire duration of the exam.
Another clinically relevant parameter in reflux disease is given by the bile content. The measurement is carried out with a fiber optic catheter that uses bilirubin as bile marker.
The only instrument available on the market for this type of measurement is the Bilitec 2000 device (http://www.cecchi.com/apparecchi-medicali/).
One of the project partner based on a CNR patent produces it.
Since then it has been used in many hospitals that considered bilimetry more and more extremely important to achieve a complete vision of the reflux pathologies.


Esophageal manometry provides information on amplitude and coordination of esophageal contractions and the relaxation and coordination of both the lower esophageal sphincter and the esophageal body.
Moreover, esophageal manometry is used in patients with GERD in order to support the diagnosis in a complex patient, to evaluate patients with atypical symptoms, to detect defective peristalsis prior to fundoplication, to exclude scleroderma or achalasia as cause of the patient’s symptoms and to assist placing of pH-probes.
The standard test takes about 30-40 minutes and it is the first to be performed in order to identify the potential necessity of a subsequent 24-hour pH-metry/bilimetry.
More recently, in some cases physicians are extending the manometry examination to 24 hours similarly to what happens for the esophageal pH-metry and bilimetry, especially when the classical short-in-time manometry does not provide sufficiently clear information on esophageal motility disorders.
In the previous manometers, the esophageal pressure was measured in correspondence of the sphincters and in a few other points along the catheter.
In the recent years, high resolution manometers capable to measure the esophageal pressure every few centimeters (down to every centimeters) provides the physicians with a more sophisticated tool capable to provide a larger spectrum of information on the esophageal motility.
Advance beyond the state-of-the-art
Attempts to develop an optical fiber pH sensor are described, with some project partners involved in the last years in a Tuscany regional project focused on the development of an optical fiber pH sensor potentially suitable to be combined with the bile sensor (http://www.cecchi.com/progetto-spes/).
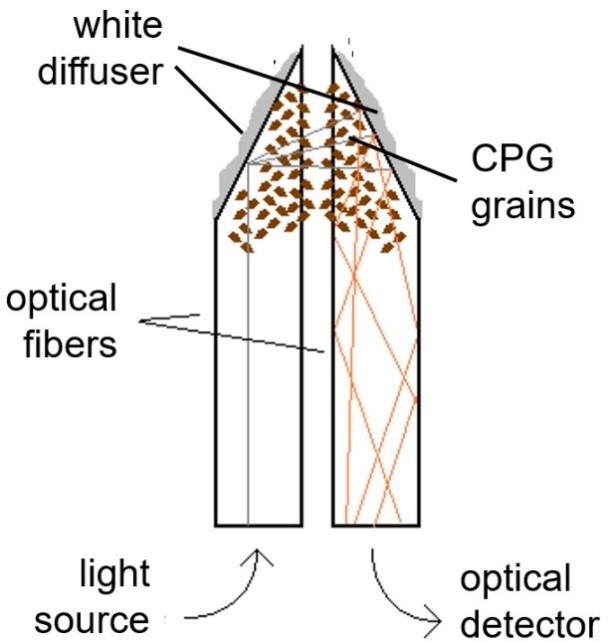
The probe shown in the Figure below makes use of controlled pore glass (CPG) grains on which the pH indicator methyl red is covalently immobilized.
The CPG grains are deposited on the lateral surface of the distal end of two 250 µm plastic optical fibers that are suitably cut to allow the light coupling between one fiber and the other, and the consequent light modulation by the pH indicator.

This probe, covered by a European patent, with the patent extension in USA under progress, was characterized in the CNR laboratory but it was never tested either on volunteers or on patients.
The development of an optical rather than electrochemical probe, utilizing optical fibers, for the detection of the gastroesophageal pH presents numerous advantages, among which the total absence of contacts or electrical wires and a potential miniaturization greater than that of the conventional micro-electrode normally used, which would lead to less stress for the patient.
None of the esophageal manometers presently used routinely by physicians makes use of optical techniques, but they are all based on the use of electrical pressure transducers.
The only optical manometers described in the literature for esophageal monitoring are those developed by one of the project partner and by the group of Prof. Arkwright (Australia), which make use of an optical fiber Bragg grating properly coated in order to detect the transversal pressure acting along the cable.
In the Arkwright design, isolated pressure transducers are used, while the approach of the project partner is to use extruder technology or injection molding technology to encase the draw tower fiber Bragg gratings with the transducer jacket, also based on the know-how and the expertise achieved in a national project previously financed.
With this technology, the manometer can be potentially low cost with the realization of the distributed sensing concept reasonably affordable.
Manometry is generally performed with sensing points every 5 cm with catheters which are not smaller than 2.5 mm, but in the case of the so-called high-resolution manometry, pressure measurement is performed roughly every cm.
It is important to observe that an optical fiber pH sensor and a fiber-based manometer are by themselves innovative products in the biomedical area for gastroesophageal applications, and they can constitute a valid alternative to the traditional devices available on the market thanks to the typical advantages of optical fibers in invasive medical applications – absence of electrical contacts and greater potential miniaturization – which leads a less discomfort and a greater safety for the patient.
However, it is their combination in a single catheter and the combination with bile probe, main objective of the present proposal, which would represent a large step-forward in the monitoring of gastroesophageal refluxes offering performances that none of the available techniques can provide.
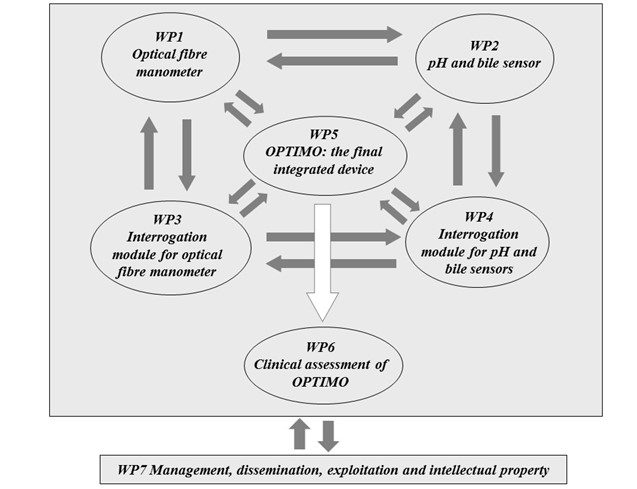
Work Plan
The Perth diagram of the project, showing the interconnections among the different work packages (WPs), is detailed in the Figure below.